

On Nov. 21, the Community Health Commission of Missouri, in partnership with the UMSL Political Science Academy hosted a town hall to discuss men’s health equity and ways to better engage our men in health advocacy for themselves and their community.
In the United States, men’s life expectancy has increased over time to 76.4 years since 1980. However, men still live 5 years less than women on average. Why is this?
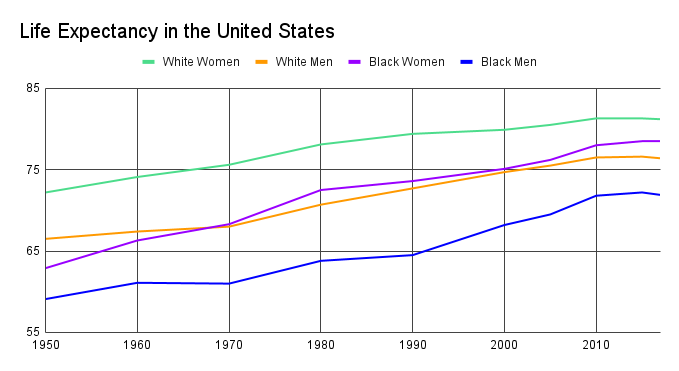
In general, men seek less preventative care than women do. Preventative care helps to detect and prevent serious diseases and medical problems before they become urgent. Men are more likely to see the doctor because of a sports injury or because of erectile dysfunction. Men also engage in riskier behaviors. In 2020, 72% of all motor vehicle crash death victims were men. More men die of diabetes and cancer than women, and the cancer mortality rate is highest among black men.
Researchers have theorized the cultural expectations to remain stoic delays men from seeking care. When you wait longer to seek care, the chances significantly increase that there will be more damage and a poorer outcome. So where do the narratives around men failing to seek care come from? Some medical circles incorrectly labeled women as “anxious” or “hysterical” for seeking medical care at a higher rate than men. In reality, women were seeking healthcare an appropriate amount and men were not going nearly enough. Men have been overrepresented in medical studies but underrepresented in clinical care.
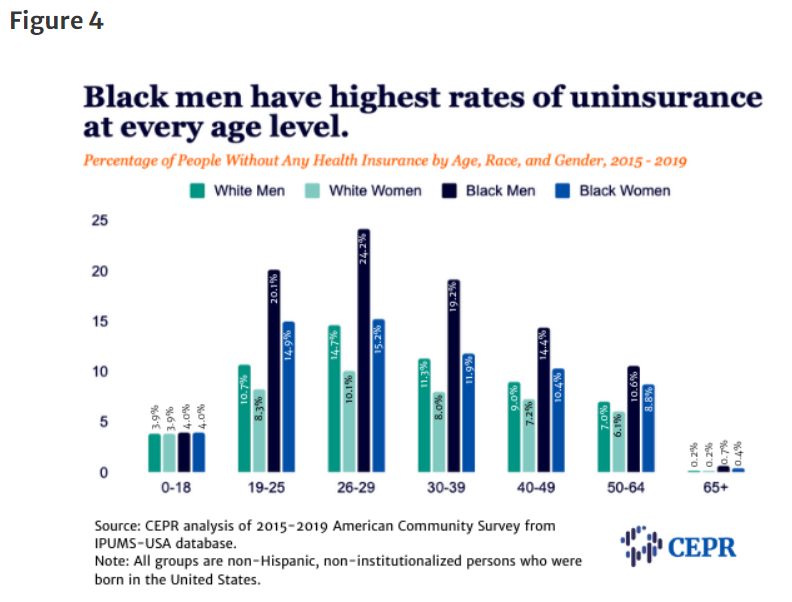
In general, men experience difficulty paying medical bills. Men may be struggling with health insurance literary levels. The uninsured rate for men is 14%, and for women the uninsured rate is 11%. Employed black men are less likely to have employer-based coverage than employed white men. The benefit inequality has widened over time. For Black men, uninsurance rates quadruple by age 19.
The Affordable Care Act and Medicaid Expansion
When Medicaid was first rolled out, most young men were ineligible for coverage. Those eligible included families and children, pregnant women, the elderly, and people with disabilities. Only some low-income people qualified. In most states, children living with income below 200% of the poverty line are eligible for Medicaid until their 19th birthday. As a result, young men’s uninsurance rates double from age 16 to age 20. Medicaid expansion allowed coverage for all people with household incomes below a certain level. This made many young men eligible for coverage.
Prior to the Affordable Care Act and Medicaid, young women paid as much as 45% more for health insurance than young men. The ACA prohibited insurers from varying premiums based on health status or gender. The ACA led to a total increase in 2014 of about $72 a month for young, healthy men ineligible for subsidies. There were also tax penalties for those without health insurance. As a result, in 2014 it was cheaper for young men to pay the penalty of not having coverage than to actually have coverage. However, coverage rose among all demographic groups after the ACA took effect.
States that have expanded Medicaid have seen positive effects among all demographics, especially men. Washington University in St. Louis estimated in 2019 that around 230,000 people in Missouri would enroll in Medicaid if it expanded. In 2021, men represented 43% of enrollees on Medicaid in Missouri, a slight dip from 44% in 2019. After the ACA was implemented, use of colon cancer screening mechanisms showed differential uptake. Studies comparing Medicaid-expansion states and states that haven’t expanded Medicaid have reported substantial improvements in preventative care screening and access. Medicaid-expanded states also diagnose and treat substantially more adults with diabetes under the age of 65. When men are covered by Medicaid, they are more likely to have a preventative care visit than men who are uninsured.
There is a significant link between losing Medicaid at age 19 and incarceration rates among young men. By their 20th birthdays, men with mental health histories are 22% more likely to have ever been incarcerated relative to men in a comparison group. Access to mental health and substance abuse services reduces arrests and incarceration rates.
Expanding Medicaid has proven beneficial for other groups as well. It increases insurance coverage rates among people with or at risk of HIV. More people are getting tested and diagnosed with HIV, and there’s more use of Pre-Exposure Prophylaxis (PrEP). There is a small but significant increase in the likelihood that men, transgender, and nonbinary individuals who have sex with men are taking PrEP to prevent HIV. Low-income adults in same-sex couples were less likely than low-income individuals in different-sex couples to have Medicaid coverage. Medicaid expansions significantly increase the likelihood that low-income men in same-sex couples reported having Medicaid by 9.8 percentage points.
Overall, expanding Medicaid helps to reduce the racial and socioeconomic inequalities in health care. Young men and older boys benefit the most from universal health care. Since the U.S. still doesn’t have completely universal health care, there are still coverage gaps for men.
Coverage Gaps for Men’s Health
Under the ACA, there are no gender-based services for men and no incentives to buy health insurance other than fines and penalties. Men are eligible for far fewer preventative services than women. For example, non-pregnant and sexually active women can receive free screenings for chlamydia and gonorrhea, but the same is not true for men. Women are also more likely to receive the HPV vaccine than men. As a result, men are 3.6 to 6 times more likely to become infected with HPV.
The ACA provides for a Well-Woman visit, with no comparable visit for men. Prostate cancer screening is not covered, but breast cancer screening is. In terms of reproductive care, condoms and vasectomies are not covered by insurance. There are also few programs or resources aimed at men and boys about preventative and reproductive health care.
Mental health is also a serious issue when it comes to men’s health. Men commit suicide at a rate 4 times higher than women. Nearly 10% of men suffer from depression, but less than half receive treatment. Schizophrenia is one of the leading causes of disability, and 90% of those diagnosed by age 30 are men. In 2021, only 40% of men with a reported mental illness received mental health services in the past year, compared to 52% of women. Research has shown that due to bias, medical providers have missed or misdiagnosed mental health illnesses in men. Some symptoms present differently for men than for women; common symptoms of depression in men includes irritability, sudden anger, increased loss of control, risk-taking and aggression.
If there is someone in your life that you are worried about, there are numerous resources to help you. Brother – You’re on My Mind is a toolkit to help start conversations about mental health and change the national dialogue regarding mental health among African American men. R U OK? helps to shape check in conversations so you feel comfortable asking the uncomfortable questions. 988 is the National Suicide Hotline, which you can call and text!
In general, men and other people with Medicaid are more likely to have other societal factors that may influence health outcomes. These include a lack of transportation, poor health literacy, and mistrust in the health care system. Not all providers even accept Medicaid, which creates another barrier. It’s important to reduce the stigma that men have to be stoic all the time, and that men need preventative health care.